Psychedelic assisted psychotherapy
I have been following the progress of PAP for some years since I first attended a lecture by Prof. David Nutt at least a decade ago. It is a tragic irony that the development of this loosely grouped substances and their utilisation for therapy was blocked comprehensively for about 50 years while the development of strategic nuclear weapons continued at pace.
It is tempting to suggest that the inexorable deterioration in weather patterns, from the careless discharge of millions of tonnes of additional CO2 and methane into our atmosphere and the actions of one malevolent dictator, threatening the use of nuclear weapons, (which would spark a nuclear winter) are explanation enough for the general disquiet, (labelled mental “illness” in (mainly) first world societies.
However the progressive darkening of our collective “zeitgeist” has more pervasive, less dramatic origins, I suggest.
My aim to offer a perspective today, which I’m more than happy to be contested. I apologise for my impaired delivery but I hope I can offer a coherent basis for why the use of psychedelic-assisted therapy may be not only imminent but essential.
Firstly I will cover the development of P.A.P in our region and what you might expect to encounter in the next decade, working in Mental Health and AOD field.
I get into conversations with clients about psychedelics approximately weekly. Many have heard of the trials of micro-dosing with LSD at Auckland Uni and the ketamine-based therapy available through Anteris…. (A trial to treat alcohol dependence with a single dose of ketamine is currently being recruited for.)
I was told by a client last week, someone who has been disabled by polydrug use, anorexia and borderline behaviour patterns for twenty years, that she had bought a pound of dried mushrooms, (.45kg.) and was working her way through 3-4g every other day. She sounds well and happy for the first time.
Secondly I will offer a point of view about the origins of, what we are told is an epidemic of mental unwellness and of substance dependence, in particular. Follow the link below for further information on the current situation in our part of the world
https://theconversation.com/why-the-tga-should-reschedule-mdma-and-psilocybin-for-the-treatment-of-mental-illness-160276#:~:text=On%20February%203%2C%20the%20TGA%20announced%20an%20interim,for%20abuse%2C%20and%20lack%20of%20suitably%20trained%20psychiatrists.
Psychedelic-assisted Psychotherapy. Lecture notes
In November of this year I attended an online conference hosted by an organisation called Mind Medicine Australia. It is a privately funded charitable organisation, dedicated to leading the development of a psychiatric treatment regime using psychedelic substances.
Their efforts are directed towards;
1) Canvassing the Australian Pharmaceutical Regulation and Classification body, the TGA,(THERAPEUTIC GOODS AUTHORITY), to change the scheduling of some psychedelic drugs so that they can be tested and evaluated.
2) Training a workforce, and developing protocols in preparation for the time when psychedelics can be used in treatment sessions.
3) Publicising the benefits of this treatment, in comparison with currently used “conventional therapies.”
It maintains and nurtures relationships with leading researchers around the world and many eminent academics in the field have been appointed “ambassadors” for MMA.
MMA was the “brain-child” of an energetic, determined couple, Tania de Jong, (AM), and Peter Hunt,(AM).(Member of the Order of Australia) who are enthusiastic psychonauts and “social entrepreneurs”. Their personal experiences and the enlightenments achieved have motivated them to make these substances available through mainstream legitimate mental health services.
Tania is a Dutch Jew ,( who believes her trauma was the result of epigenetics and her ancestors experience of persecution, an accomplished soprano and “creative alchemist” and Peter is described as a philanthropist and investment banker.
They are both passionate about the organisation and its goals.
Mental Health. (“An urgent and serious need”).. Tania de Jong.
The incidence of depression, anxiety has been increasing steadily over the last forty years.
WHO data:
..between the years 1990 and 2013, the number of people suffering from anxiety and depression increased to 615 million from 416 million, which equates to an almost 50% increment. Nearly 10% of the global population is affected, with mental illnesses making up 30% of the world’s non-fatal disease burden.
20% Australian adults have chronic mental illness.12% are on antidepressants including 25% of Australians over 60 years of age. ( 18% increase in past five years) 95% increase in last 15 years.
More than 45% will experience mental illness in their lifetime.
A 2016 WHO study concluded that anxiety and depression disorders cost the world as a whole nearly US $1 trillion every year yet $4 trillion was made by pharmaceutical companies to ‘treat’ these diseases
There have been no significant advances in treatment for the last fifty years and even the substances being considered now were all described in the first half of the last century,
The Origin of Mental “Illness”. The Pernicious Influence of Early Trauma.
I credit Gabor Mate with this hypothesis, or “model”
The human infant has an extremely long period of dependence and helplessness. To ensure they remain protected they need secure attachment to, ( at least), one capable adult, on whom ,they instinctively understand, they are reliant. Secure attachment is. primary survival need.
A second “need” can be labelled “authenticity”, ie, feeling able to “trust their gut”.. When threatened, they are wired to respond automatically and they need to believe that their automatic reaction was the right response and build trust in their judgement.
But what happens if their response is not acceptable to their attachment figure.?
If they detect that their automatic reaction causes irritation and threatens their protection, they will sacrifice authenticity, in return for retaining the approval of that protector and will continue to adjust their behaviour to what they perceive to be expected. But this is not always obvious, may not get consistent results. Uncertainty becomes anxiety.
The amygdala, that nugget in the base of the brain, is the area that processes reactions to threat, (flight or freeze, resisting is rarely an option). It lights up then dims slowly as the crisis passes. If it is not resolved ,with appropriate soothing, the amygdala remains aroused and continues to flood the system with stress hormones and this is experienced as anxiety ..prolonged fear.
If this hyper arousal persists the amygdala remains habitually hyperactive and hence the infant experiences chronic anxiety. This is disabling, distracting and impairs cognitive performance. As it self-perpetuates it eventually progresses to a label of depression and substance, (or behavioural ), addiction.
( on the way, they are likely to attract other interim labels, oppositional defiant disorder, attention deficit hyperactivity disorder, dyslexia)
In its mildest form it results in poor self-esteem,(self image), low self-confidence, (self efficacy), social phobia and imposter syndrome.
Behavioural traits, become exaggerated and impede social development and there is strong possibility of a diagnosis of personality disorder.
Inadequate attachment and PTSD.
Parenting, providing 24/7 attention to infant’s needs requires an absolute, selfless, commitment.As a species we have lived and thrived as small communities with common goals. Parenting was shared between multiple adults. We have not adapted to the suburbanisation that followed the industrial revolution.
Supports that have evolved are inequitably distributed, to the higher decile areas, where they can afford them.
A common history amongst most of those with this narrative is that they describe re-experiencing, in some format ,distressing episodes, whether it be re-imagining specific events or just the associated evoked emotions.
This is highly correlated with a propensity to ruminate,,to experience an internal monologue which is persistent and negative and becomes conscious when the brain is not distracted with other more complex tasks… see default mode network
So the bundle of remembered, and “ re-experienced”, frightening episodes, whether it be a single terrifying event, or a countless number of abusive events, both observed and endured,,this narrative history is the product of an incompletely resolved memory.. it evokes an unmodulated fear which leads to the desire to self-medicate.
This is a post-traumatic stress disorder
So, QED.
Excluding degenerative disorders, psychotic disorders and other wiring problems like autism spectrum disorder., Axis I disorders can be characterised as PTSD. ( from infant neglect to battle fatigue.)
The intensity of the recollection exceeds the ability to deal with it.
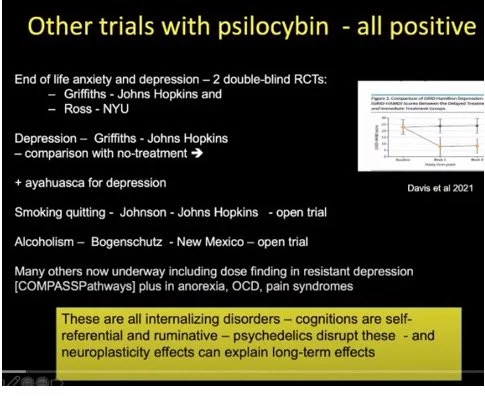
And psychedelic assisted psychotherapy works.
MDMA and PTSD.
There are two subtypes of PTSD.
Nondissociative.
The amygdala is chronically over active and the prefrontal cortex is underactive
Dissociative.
Considered even harder to treat with conventional therapy. The amygdala is underactive, and the cortex overactive, causing emotional numbing and fragmentation of personality.
https://www.nature.com/articles/s41591-021-01336-3
This is a link to the study which established the effectiveness of MDMA with certainty.
Phase 3. Randomised, double blind, placebo controlled study.
The study used a rigid protocol, extending over 18 weeks.It used three medicated sessions interspersed with three session of preparation before the first then three sessions of integration between each dose.
Slide on protocol
37%, placebo group no longer met criteria at end of trial
67% of the medication group responded and a further 21% made significant gains.
Both types responded and the change was sustained .
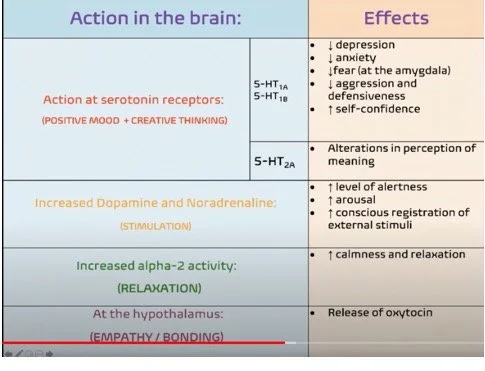
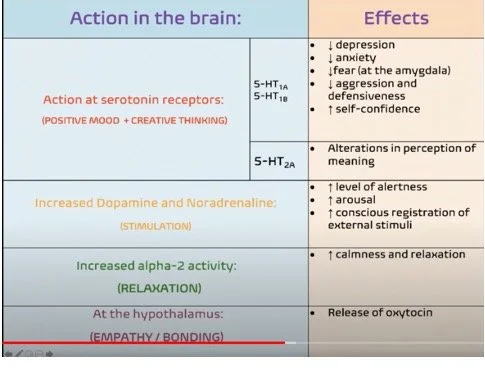
Mechanism of Action of MDMA
MDMA acts on at least three separate systems. Firstly it is partially active at the 5-HT 2a receptor, it increases the release of serotonin and is variably psychedelic,. The amphetamine part stimulates the norepinephrine pathways and it releases oxytocin, the sum effect being, a bit trippy, quite stimulating and relaxing at the same time.
Slide on mechanism of action
There are reported to be 3-400 private companies working on development of a commercial product, challenging patents, synthesising new analogues. Said to have raised $1.5 billion US.
Risk is that these companies are focussing on the medication, not the therapy. It is likely there will be a backlash when these inappropriate regimes return a bad record of responses.
MDMA and Alcohol Dependence.
Pilot study..
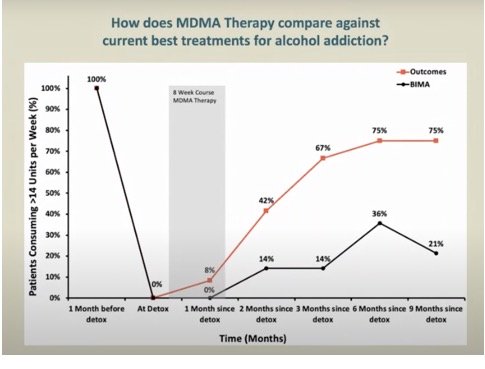
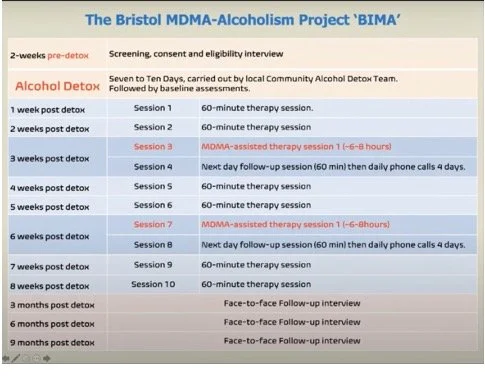
This was an open label study to establish safety and tolerability. It involved only 14 subjects recruited from local drug treatment centre.
difference in results were striking. Furthermore there was no "come down" after the treatment in fact people's mood remained relatively elevated.
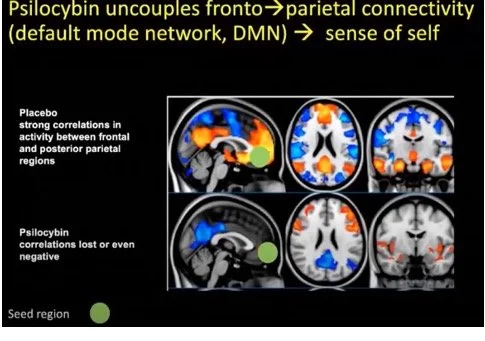
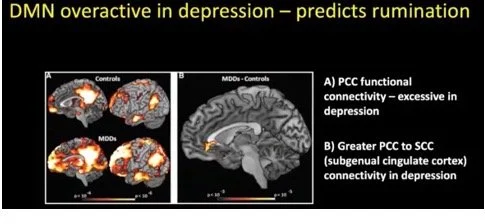
The Default Mode Network.
David Nutt’s group at Imperial College have led the world in functional MRI imaging to elucidate the effect of the tryptamines namely psilocybin, because its half life is manageable. Ibogaine and Ayahuasca are in the same group but unpleasant to take.
The DMN is a “circuit” between the anterior and posterior cingulate gyra and also includes a parieto-temporal component. It is most active when the owner is at rest, day-dreaming or ruminating. It is what the brain does when there is no more urgent demands for its attention.
It is the location of the sense of self, the “ego”, the internalised conception of who we are.
It is the notional nidus of the classic negative commentary..” I’m a failure, everybody knows I’m a failure, “ etc.
It is the nagging negative internal monologue that leads people too seek relief by self-medicating with intoxicants.The severity of depression correlates very well with the intensity of rumination and that correlates with hyperactivity of the DMN.
For example, the unresolved trauma of PTSD will replay when the brain is resting.
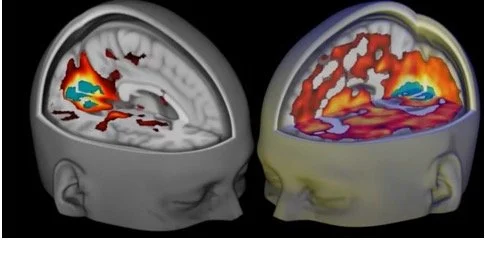
Psilocybin blocks the function of the DMN and results in stimulation of the 5HT2A receptors.
These receptors are recent arrivals in the evolution of the mammalian brain and are most concentrated in the “level 5”.pyramidal cells in the deep cortex. The decreased connectivity of the DMN leads to the reduced processing of incoming sensory stimuli and it is suggested that it is perceived in un filtered, primitive form, eg the visual patterns approximate those seen by infants
The Perils of “Higher” Consciousness
I struggled manfully to mine the terabytes of weapons-grade bullshit written about the nature of consciousness. ,(which the French call “conscience”)
After trying to pronounce, let alone understand words such as “epiphenomenalism” and “eliminativist”
This is how one such paper concluded..
The buttock, however, in man, is different from all animals whatsoever. What goes by that name, in other creatures, is only the upper part of the thigh, and by no means similar.
George Louis Leclerc de Buffon (1792, pp. 80–81)
Why do people think? Why do they calculate the thickness of walls of a boiler and do not let the chance determine it? Can a calculated boiler never explode? Of course, it can. We think about actions before we perform them. We make representations of them, but why? We expect and act according the expectancy;… Expectancy [is] a preparatory action. It outstretches its arms like a ball player, directs its hands to catch the ball. And the expectancy of a ball player is just that he prepares arms and hands and looks at the ball.
Ludwig Wittgenstein (1996, pp. 109, 139)
I wonder if the issue can be viewed much more simply..All the complexity of morality and mortality and how they interact can be assumed to be due to basic human instinct.. the drive to survive and in particular a fear of death, the dreaded end.
Ubiquitous and consistent across all the, otherwise diverse ,cultures of the world have developed organised religious rituals in the service of, superhuman, ( and therefore unseeable), all seeing beings, who promise, if one is adherent to the rules, the avoidance of termination.
Some of these rituals have used psychedelic experiences as a normal part of their religious practice.
Buddhist meditation practices, focussing on “letting go” of negative thoughts by distancing from them and examining them critically, has been adapted and is advocated widely in Western mental health practices. This occasionally leads to an ecstatic experience that the person experiences as, at least, a major new insight and lasting change of perspective, and often as a mystical, spiritual experience, which emphasises connectedness and a feeling of “oneness” with the w orld..
Some Western, Christian traditional churches put considerable emphasis on the ecstatic experience, when during feverish group worship, the person is entered by God, or his understudy.
I believe these similarities are examples of human behaviour evolution aimed at a spiritual elevation, reassurance of the existence in a “higher consciousness” and it is the same experience that is caused by psychedelic substances, obviously vastly more efficiently and predictably.
Bill Richards, the doughty veteran of Johns Hopkins, who has devoted his life to researching psychedelics.. has surveyed online volunteers to answer questions, about their spiritual beliefs and found that there was a two point up-tick, (on scale of 1:10), after a psychedelic experience, in mystical beliefs; for example, being open to possibility that objects previously considered inanimate, may be conscious.
This emphasis on mystical experience, is shared by many of the most enthusiastic promotors of PAP. Bill Richards d3voted one of his sessions to the choice of background music for the session ( Brahms is preferred)… Tania de Jong AO promoted a CD of her self singing opera.
It remains a moot point whether by taking the trip out of the spiritual underworld, you can keep the spirit world out of the trip.. I think not..
The New World.. who will be the Brave..
Point 1.
The cultural zeitgeist insists that we are becoming unhappier. Politicians and parents clamour for better outcomes in our “mental Health” statistics.
In fact nothing new has been introduced in fifty years or more and results of these treatment approaches are modest and nobody is fooled.
The increase in “mental health problems” is an increase in “life distress”
Namely anxiety, depression, resultant substance abuse, behavioural addictions, cluster b. Personality “exaggeration”.
These conditions can all be conceptualised as PTSD, namely the residual distress and dysfunction from inadequate attachment and home circumstances in the pre-conscious brain, in particular the midbrain and amygdala, where memories which are inaccessible later in life , of experiences which frightened and in the long term created unbalanced pathways to the prefrontal cortex,
These pathways are largely inaccessible and immutable by any other treatment modalities,,
That these events are not amenable to change because of intergenerational transmission of parenting plus unchangeable social circumstances.
How can this new approach to therapy be ignored..it won’t be.
What should we do..
Focus on Mdma.
Parkinson’s and me.
I signed up early for my diagnosis.. At Med School I was fascinated by the nervous system...But I was the worst kind of hypochondriac and formulated quite a number of wrong self-diagnoses over the following years,…. but when I was just shy of 60 the left arm stopped swinging. Combined with my near complete anosmia, I knew the game was up..
But then, gradually but inexorably, a real “awakening”, began..with things that I hadn’t anticipated, that don’t get described.. pervasive global anxiety.. and emotional fragility, tears abruptly welling up from the chest and overflowing from the eyes..insidious loss of stamina, weakness and exhaustion, that was soon labelled depression.. because loss of enjoyment looks like sadness..and the sweating, dribbling , dripping sweat, even in the palms of the hands, making reaching out a self-conscious act.
And then you’re off.. climbing the “treatment” step-ladder, doses increase , new drugs are introduced Tremulously holding your finger in the dyke , you imagine the dopamine producing cells deep in the brain depleting, on a predestined timetable, condemned without explanation.
But the effects of the drugs are lumpy, uneven and hard to predict..fluctuating like a sine wave. At the bottom of the curve, I am stiff and tremulous. Walking is like wading through an invisible miasmic swamp , the air pushes back, the ground is perpetually uphill. At the top, at the peak of the wave ,all my limbs writhe, and like a frustrated octopus, shocked at the size of his latest utilities bill, I gesticulate incomprehensibly, to the obvious discomfort of others.
Its the most exhausting stage of the cycle. The urge to move is irresistible, pointless, grotesque.. With intense concentration you find you can control it but as soon as you focus elsewhere, it’s back.
So you try to keep the effect in the “mid-zone”.. limit the oscillations to between the two tropics as it were, in the sweet spot, the temperate zone.
Feelings, like smells and tastes, become memories. Some emotions you farewell with no nostalgia. Anger and resentment are buried in the subsoil of your mid-brain, beneath a crust of apathy. Increasingly you realise that the urge to contribute, to participate ,at meetings and “functions”,has been replaced by neutral observation. You catch yourself nodding periodically, without any conscious intention to agree, as if, maybe, by some primitive social reflex, your mid-brain is playing along, to avoid appearing detached.
And of course ,you are warned, there’s the potential for more spectacular, drug-induced aberrations.The longer and harder you chemically stimulate a pleasure pathway, apparently, the more you risk a cataclysmic response. Like poking a hibernating nest of bumble-bees with a stick, eventually you may be stung by a grotesquely exaggerated desire for the reckless pursuit of excitement ,(or over-valued novelty.)
Soon, one realises, you are obliged to start looking round for something to sweeten the deal. A constant diet of the dough of disappointment sits unleavened in the craw, threatening to drag you below the point of no recoil. My sense of wobbly forward momentum is preserved by work.. Less from the clients I get to know, although the capacity of some to maintain hope is admirable, but more from the strong working relationships that have grown steadily over the last twenty years. As my age and overt physical anomalies have advanced I have come to appreciate more and more the respect and warmth I feel from my colleagues, no more obviously demonstrated by the efforts they mede recently to acknowledge my 70th birthday.
My birthday was an event drawn out much longer than the single day and it also served to remind me of how lucky I am to be surrounded by a wife and family who care for me. It was the best, most memorable anniversary that I can remember and I would not swap it for anything.
The future is a foreign land and I must take pains to pack adequately for the trip, to adapt continually to the vagaries of my involuting brain. I believe that some illusion of progress is essential to retaining hope and I take much pleasure in observing the dynamic development of my children and their children. Good fortune has determined that my intellect has not been eroded at a rate any greater than the average septuagenarian.
But nonetheless I’m aware of my subconscious, or maybe more correctly, my almost-conscious discomfort , my own private poke in the ear from an umbrella-wielding Jiminy of my own creation..reminding me that as time passes now the end comes into view with ever-sharpening focus, even though the manner of its arrival remains a mystery. I am more likely to accept the manufacturer’s assertion of a lifetime guarantee.
In the pocket of my sensible denims, ( R M Williams, good quality, they’ll “see me out”) I have a sensible `silk purse.. I made it myself from a sow’s ear I swapped years ago for the handful of magic beans I was given as a child..( I have let go of the belief that I was tricked out of them). I just have to make sure I continue to look after the contents.
Update 19 September 2024
It’s the second Thursday I have been on leave in Matapouri with my wife and dear friends.
I have decided to write a diary.. A check-in yearly to assess progress.. at worst it may amuse, at best it may serve as a record of a progressive dementing disease.
Timeline to date:
2002. noticed involuntary tremor of left hand while dancing
“too early to diagnose Parkinson’s Disease.”
2005-2010., intrusive anxiety, tendency to over-reaction of sympathetic system, sweating, tremor, warm periphery, sweaty palms., runny nose.
Restless legs became a nightly affliction preventing sleep for ,up to an hour
Increasing tendency to hang left arm when walking. Increasing awkwardness of left (dominant) hand. Buttoning up a shirt becomes an increasingly fumbling slow process.
All fine movements are affected
2011 diagnosed and started on Amantadine then L-dopa
Commenced on different anti-depressant, Venlafaxine
Became depressed in middle of 2014, following a very painful disc prolapse.
Required to attend a psychiatrist to reassure the Medical Council. Started Escitalopram..gradual lifting of mood.
Psychiatrist now wants me to go for cognitive test.
Starting to hold left hand like a broken wing and doing much more with right hand.
Current Baseline,(at my best as a result of holiday)
I am three kilos of abdominal fat overweight, in spite of which there is now very obvious wasting of dorsal, arm and leg muscles so my overall weight hasn’t changed much.
I have exercised for several hours on a mountain bike most days and had a distinct improvement in strength and stamina but I am still globally weak and my left arm becomes leaden and disconnected, floppy yet stiff, aching
Able to ride the old Coach Road circuit with Rick and possibly as fast as when we did it ten years ago,(in the other direction on worse roads). Can sustain 120 bpm and peak at 140 for short bursts.
Sweating is torrential during exercise and otherwise grossly excessive especially when under stress.
Tremor can become irrepressible when stressed. Varies markedly day to day and fluctuates through the course of the day. I take midday meds and sometimes not .. I have never identified an association with my symptom level, but I’m much more likely to take daytime meds if I’m having a bad day with the movement problems. I have jerking dystonia of left foot which is sometimes there and sometimes not.
My memory of past events long and short seems normal
I have frequent difficulty with word-finding which is a matter of great sadness to me.
I have the usual’ Zone-out” can’t remember your name”, moments as I believe is so common as to be normal.
I feel I have become more detached and uninterested in social gatherings. I seem happy to observe. If engaged by a stranger I am disabled by my sweating, tremor and awkwardness.
My sleep is adequate whether or not I use the CPAP mask. I wake generally twice. It can take meditation and relaxation to get back to sleep. The dreams are the mostly complete narrative and very vivid..often involving strangers.. Also strangely frequent failure in self-management in school or Med School
My back, is a train wreck and I get stiffness and a few butt-aches daily.
My core strength has deteriorated from pain and disuse. I must use my arms and legs together to rise from sitting.
It seems to be mainly weakness in both thighs. Both have wasted markedly.
My bowel is now accustomed to a daily double dose of Macragol and electrolytes and I am rewarded most days.
I have a dry mouth all the time.. should chew gum continually but bad look at work I think.
At work I am managing very well dealing with a difficult situation effectively and decisively. I am well-respected at work except by a problematic relationship with two colleagues. I frequently have ben thinking about work when lying awake at night. I am able to handle several situations concurrently and have not had to resort to the..”one thing at a time..” strategy
So far then the biggest losses have been physical, the weakness , easy exhaustion and poor balance. It is difficult to mountain bike on narrow tracks and I overbalance or lose my control frequently. My only solution is to keep exercising.
I have to consciously lengthen and speed up my stride and arm swing.. I commonly catch myself tottering.
As well as this I am very conscious of the deterioration of fine control in my left hand..the hand is becoming increasingly naïve, forgetting it once automatically undid knots, pegged out washing, did up buttons, opened packaging., Each attempted fine task is an exercise in training the fingers to do what they used to do automatically. And the fingers do not learn , they approach every task as if they have encountered it for the first time.
Written April 2015
It’s the second Thursday I have been on leave in Matapouri with my wife and dear friends.
I have decided to write a diary.. A check-in yearly to assess progress.. at worst it may amuse, at best it may serve as a record of a progressive dementing disease.
Timeline to date:
2002. noticed involuntary tremor of left hand while dancing
“too early to diagnose Parkinson’s Disease.”
2005-2010., intrusive anxiety, tendency to over-reaction of sympathetic system, sweating, tremor, warm periphery, sweaty palms., runny nose.
Restless legs became a nightly affliction preventing sleep for ,up to an hour
Increasing tendency to hang left arm when walking. Increasing awkwardness of left (dominant) hand. Buttoning up a shirt becomes an increasingly fumbling slow process.
All fine movements are affected
2011 diagnosed and started on Amantadine then L-dopa
Commenced on different anti-depressant, Venlafaxine
Became depressed in middle of 2014, following a very painful disc prolapse.
Required to attend a psychiatrist to reassure the Medical Council. Started Escitalopram..gradual lifting of mood.
Psychiatrist now wants me to go for cognitive test.
Starting to hold left hand like a broken wing and doing much more with right hand.
Current Baseline,(at my best as a result of holiday)
I am three kilos of abdominal fat overweight, in spite of which there is now very obvious wasting of dorsal, arm and leg muscles so my overall weight hasn’t changed much.
I have exercised for several hours on a mountain bike most days and had a distinct improvement in strength and stamina but I am still globally weak and my left arm becomes leaden and disconnected, floppy yet stiff, aching
Able to ride the old Coach Road circuit with Rick and possibly as fast as when we did it ten years ago,(in the other direction on worse roads). Can sustain 120 bpm and peak at 140 for short bursts.
Sweating is torrential during exercise and otherwise grossly excessive especially when under stress.
Tremor can become irrepressible when stressed. Varies markedly day to day and fluctuates through the course of the day. I take midday meds and sometimes not .. I have never identified an association with my symptom level, but I’m much more likely to take daytime meds if I’m having a bad day with the movement problems. I have jerking dystonia of left foot which is sometimes there and sometimes not.
My memory of past events long and short seems normal
I have frequent difficulty with word-finding which is a matter of great sadness to me.
I have the usual’ Zone-out” can’t remember your name”, moments as I believe is so common as to be normal.
I feel I have become more detached and uninterested in social gatherings. I seem happy to observe. If engaged by a stranger I am disabled by my sweating, tremor and awkwardness.
My sleep is adequate whether or not I use the CPAP mask. I wake generally twice. It can take meditation and relaxation to get back to sleep. The dreams are the mostly complete narrative and very vivid..often involving strangers.. Also strangely frequent failure in self-management in school or Med School
My back, is a train wreck and I get stiffness and a few butt-aches daily.
My core strength has deteriorated from pain and disuse. I must use my arms and legs together to rise from sitting.
It seems to be mainly weakness in both thighs. Both have wasted markedly.
My bowel is now accustomed to a daily double dose of Macragol and electrolytes and I am rewarded most days.
I have a dry mouth all the time.. should chew gum continually but bad look at work I think.
At work I am managing very well dealing with a difficult situation effectively and decisively. I am well-respected at work except by a problematic relationship with two colleagues. I frequently have ben thinking about work when lying awake at night. I am able to handle several situations concurrently and have not had to resort to the..”one thing at a time..” strategy
So far then the biggest losses have been physical, the weakness , easy exhaustion and poor balance. It is difficult to mountain bike on narrow tracks and I overbalance or lose my control frequently. My only solution is to keep exercising.
I have to consciously lengthen and speed up my stride and arm swing.. I commonly catch myself tottering.
As well as this I am very conscious of the deterioration of fine control in my left hand..the hand is becoming increasingly naïve, forgetting it once automatically undid knots, pegged out washing, did up buttons, opened packaging., Each attempted fine task is an exercise in training the fingers to do what they used to do automatically. And the fingers do not learn , they approach every task as if they have encountered it for the first time.